Blood supply to the hip
Infant – Nutrient arteries (A) are clear in each part of hip bone with periosteal arteries developing later.
Pubis = Periosteal anastomosis from Obturator, Inferior Epigastric & Medial Circumfelx Femoral (MCF) A’s.
Ilium = Iliolumbar A branches enter nutrient foramina. Superior Gluteal, Obturator & Superficial Circumflex Iliac A’s provide periosteal supply.
Ischium = Obturator, MCF & Inferior Gluteal A’s.
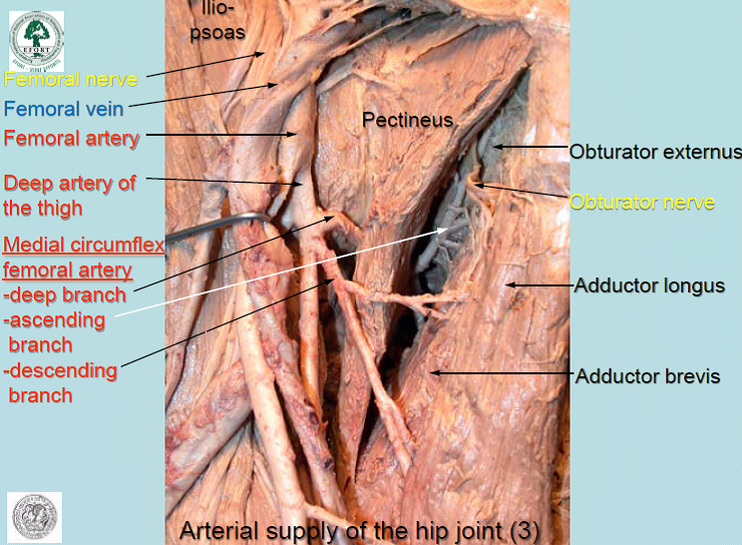
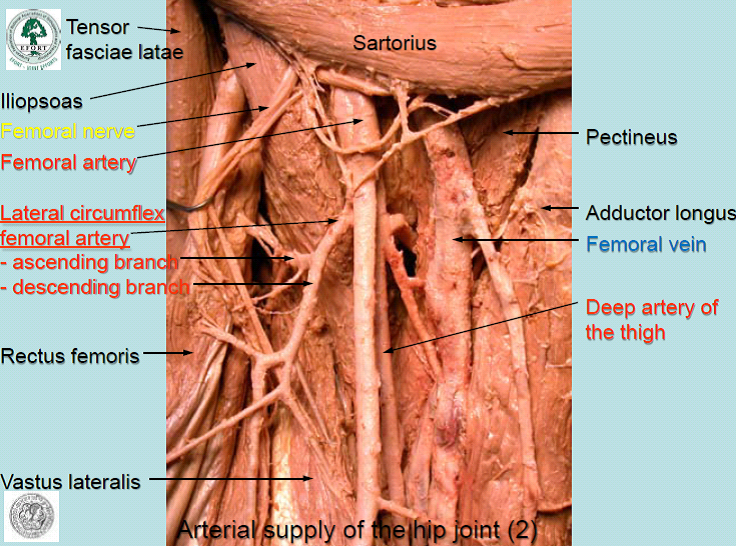
Femoral Head =Arterial ring outside of fibrous capsule. MCF, LCF and Sup. & Inf. Gluteal A’s.
Trochanteric Anastomosis = Near Trochanteric Fossa. Ascending branch of MCF and descending branches of Sup. & Inf. Gluteal A’s. Form retinacular vessels that pierce capsule and ascend neck of femur, providing main supply to the head.
Cruciate Anastomosis = Level with lesser trochanter. Transverse branches of MCF & LCF, descending branch of Inf. Gluteal and branch of 1st perforating A (of Profunda Femoris).
Cervical branches (from MCF, Sup. & Inf. G A’s) pierce the hip capsule and ascending the neck becoming retinacular arteries that form a sub-synovial intra-capsular anastomosis.
Ascending cervical A’s give off metaphyseal branches that enter the neck. The intra-capsular ring gives off Lat. & Inf. Epiphyseal branches.
Small Med. Epiphyseal supply, important during childhood, reaches head along ligamentum teres from acetabular branches of Obturator & MCF A’s. Anastomose with other epiphyseal vessels.
During growth the epiphyseal and metaphyseal branches are separated by the epiphyseal plate. The anastomoses of the head forms after osseous union of head and neck. The ephiyseal plate and therefore epiphysis is vulnerable to injury.
Perthe’s Disease = Osteochondritis of the head of the Femur. Can lead to deformity of the head of Femur and/or of the acetabulam. Characterised by idiopathic avascular osteonecrosis of the femoral epiphysis leading to an interruption of the blood supply to the head of the femur. Typically affects young children and can be a precursor to OA in adulthood.
Originally though to be caused by an interuption to blood supply (Legg), Rickets (Calve) or infection (Perthes). Currently, a number of factors have been implicated including heredity, trauma, endocrine, inflammatory, nutritional, and altered circulatory haemodynamics. Risk factors include impaired and disproportionate growth, low birth weight, delayed skeletal maturity, short stature and systemic hormonal changes.
No specific cause has been identified but there is a reduction in blood supply to the head of the Femur. The A of the ligemantum teres is constricted or blocked before the MCF A can take over the supply. Femoral head disfigurement (flattening/collapse) occurs between 4-10years, usually boys.
S&S – Hip, knee or groin pain. Decreased ROM, antalgic/uneven gait, LLD and disuse atrophy of thigh mm.
Pubis = Periosteal anastomosis from Obturator, Inferior Epigastric & Medial Circumfelx Femoral (MCF) A’s.
Ilium = Iliolumbar A branches enter nutrient foramina. Superior Gluteal, Obturator & Superficial Circumflex Iliac A’s provide periosteal supply.
Ischium = Obturator, MCF & Inferior Gluteal A’s.
Femoral Head =Arterial ring outside of fibrous capsule. MCF, LCF and Sup. & Inf. Gluteal A’s.
Trochanteric Anastomosis = Near Trochanteric Fossa. Ascending branch of MCF and descending branches of Sup. & Inf. Gluteal A’s. Form retinacular vessels that pierce capsule and ascend neck of femur, providing main supply to the head.
Cruciate Anastomosis = Level with lesser trochanter. Transverse branches of MCF & LCF, descending branch of Inf. Gluteal and branch of 1st perforating A (of Profunda Femoris).
Cervical branches (from MCF, Sup. & Inf. G A’s) pierce the hip capsule and ascending the neck becoming retinacular arteries that form a sub-synovial intra-capsular anastomosis.
Ascending cervical A’s give off metaphyseal branches that enter the neck. The intra-capsular ring gives off Lat. & Inf. Epiphyseal branches.
Small Med. Epiphyseal supply, important during childhood, reaches head along ligamentum teres from acetabular branches of Obturator & MCF A’s. Anastomose with other epiphyseal vessels.
During growth the epiphyseal and metaphyseal branches are separated by the epiphyseal plate. The anastomoses of the head forms after osseous union of head and neck. The ephiyseal plate and therefore epiphysis is vulnerable to injury.
Perthe’s Disease = Osteochondritis of the head of the Femur. Can lead to deformity of the head of Femur and/or of the acetabulam. Characterised by idiopathic avascular osteonecrosis of the femoral epiphysis leading to an interruption of the blood supply to the head of the femur. Typically affects young children and can be a precursor to OA in adulthood.
Originally though to be caused by an interuption to blood supply (Legg), Rickets (Calve) or infection (Perthes). Currently, a number of factors have been implicated including heredity, trauma, endocrine, inflammatory, nutritional, and altered circulatory haemodynamics. Risk factors include impaired and disproportionate growth, low birth weight, delayed skeletal maturity, short stature and systemic hormonal changes.
No specific cause has been identified but there is a reduction in blood supply to the head of the Femur. The A of the ligemantum teres is constricted or blocked before the MCF A can take over the supply. Femoral head disfigurement (flattening/collapse) occurs between 4-10years, usually boys.
S&S – Hip, knee or groin pain. Decreased ROM, antalgic/uneven gait, LLD and disuse atrophy of thigh mm.