HEADACHES
Red Flags
ƒ. New onset or change in headache in patients who are aged over 50
ƒ. Thunderclap: rapid time to peak headache intensity (seconds to 5 mins)
ƒ. Focal neurological symptoms (eg limb weakness, aura <5 min or >1 hr)
ƒ. Non-focal neurological symptoms (eg cognitive disturbance)
ƒ. Change in headache frequency, characteristics or associated symptoms
ƒ. Abnormal neurological examination
ƒ. Headache that changes with posture
ƒ. Headache wakening the patient up (NB migraine is the most frequent cause of morning headache)
ƒ. Headache precipitated by physical exertion or valsalva manoeuvre (eg coughing, laughing, straining)
ƒ. Patients with risk factors for cerebral venous sinus thrombosis
ƒ. Jaw claudication or visual disturbance (GCA)
ƒ. Neck stiffness (meningitis)
ƒ. Fever (Infection)
ƒ. New onset headache in a patient with a history of human immunodeficiency virus (HIV)infection
ƒ. New onset headache in a patient with a history of cancer
ƒ. Thunderclap: rapid time to peak headache intensity (seconds to 5 mins)
ƒ. Focal neurological symptoms (eg limb weakness, aura <5 min or >1 hr)
ƒ. Non-focal neurological symptoms (eg cognitive disturbance)
ƒ. Change in headache frequency, characteristics or associated symptoms
ƒ. Abnormal neurological examination
ƒ. Headache that changes with posture
ƒ. Headache wakening the patient up (NB migraine is the most frequent cause of morning headache)
ƒ. Headache precipitated by physical exertion or valsalva manoeuvre (eg coughing, laughing, straining)
ƒ. Patients with risk factors for cerebral venous sinus thrombosis
ƒ. Jaw claudication or visual disturbance (GCA)
ƒ. Neck stiffness (meningitis)
ƒ. Fever (Infection)
ƒ. New onset headache in a patient with a history of human immunodeficiency virus (HIV)infection
ƒ. New onset headache in a patient with a history of cancer
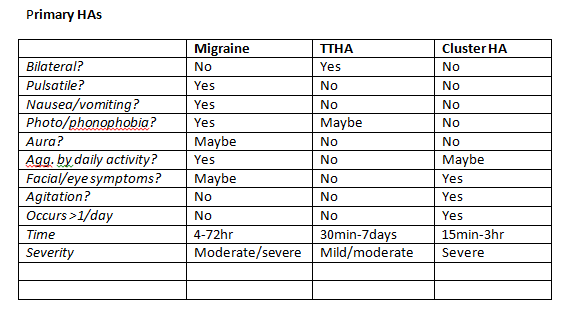
Primary Headaches
1. Migraine
With or without aura (without most common).
Without = Idiopathic recurring headache disorder with attacks lasting 4-72hours.
Unilateral, pulsating quality, moderate/severe intensity, aggravated by physical activity and associated with nausea/vomiting, photo- and phonophobia. Must have occurred on 5 occasions.
Caused by sensitivity of vessels in the brain to various triggers leading to vapid changes in vessel diameter – constriction followed by dilation = pulsating quality. Changes in blood composition and platelet function endogenously or environmentally play a role in triggering them. May be associated with the menstrual cycle.
With = Idiopathic, recurring disorder with attacks of neurological symptoms localised to the cerebral cortex or brain stem, usually developing over 5-20min and lasting 60min. HA, nausea, and/or photophobia follow the aura. HA may last 4-72hr or may be absent.
Typical aura = Unilateral visual disturbance, hemisensory symptoms, hemiparesis or dysphasia or any combination of these.
Regional cerebral blood flow is decreased (to area corresponding with symptoms), usually starting posteriorly and spreading anteriorly. Reduction in blow flow in usually above or at ischemic threshold and rarely below. Gradual transition to hyperaemia occurs in the same area (not related to the HA).
Can be difficult to distinguish from tension HA but are usually unilateral.
2. Tension-type headache (TTHA)
Recurrent episodes of HA lasting minutes to days. Typically pressing/tightening in quality, mild/moderate intensity, bilateral, not worsened with routine physical activity. Nausea and vomiting are absent but photo- and/or phonophobia may be present. Can be episodic or chronic, which can be extremely disabling. Peripheral pain mechanisms play a role in episodic TTHA, whereas central mechanisms are involved with chronic TTHAs.
Infrequent episodic TTHA = < 12/year. No nausea/vomiting. Some photo/phonophobia. 30min to 7days.
Frequent episodic TTHA = >12 but <180 days/year. No nausea/vomiting. Some photo/phonophobia. 30min to 7days. With or without pericranial muscle tenderness (temporalis, masseter, medial and lateral pterygoids, SCM, splenius capitis, sub-occipitals and trapezius).
Chronic TTHA = HA occurring >15days/month for more than 3months or >180days/year. (Episodic can progress to chronic). No nausea/vomiting. Some photo/phonophobia. 30min to 7days.
Exact mechanisms are unknown but they are related to involuntary tightening of muscles induced physically or mentally. Generally considered to be psychogenic but more severe types may also have a neurobiological basis.
Is the most common type of primary HA, occurring in 30-78% of the population
3. Cluster headache / chronic paroxysmal hemicrania
Cluster HA = Severe, unilateral pain that is orbital, supraorbital, temporal or any combination, lasting 15min to 3hrs, up to 8 times per day. Often associated with; unilateral conjunctival infection, lacrimation, nasal congestion, rhinorrhoea, forehead and facial sweating, miosis, ptosis, eyelid oedema and restlessness/agitation.
Occur in periods that may last weeks or months and are separated by periods of remission lasting months or years - 10-15% experience chronic symptoms without remission.
During a cluster period attacks may be provoked by alcohol, histamine or nitroglycerine. Pain can be excruciatingly intense with the patient unable to lie down. Pain invariably recurs on the same side.
Paroxysmal Hemicrania = Attacks with similar characteristics to cluster Has but more frequent, shorter lasting, more common in females and respond absolutely to indomethacin (NSAID).
At least 20 attacks of severe unilateral orbital/supraorbital/temporal pain lasting 2-30min. Associated with conjunctival infection, lacrimation, nasal congestion, rhinorrhoea, forehead and facial sweating, miosis, ptosis, eyelid oedema and restlessness/agitation. Five attacks per day.
4. Miscellaneous headaches not associated with structural lesion
Stabbing HA = Transient and localised stabs of pain in the head that occur spontaneously in the absence of organic disease of underlying structures or of the cranial nerves.
Predominantly felt in the distribution of the ophthalmic branch of the trigeminal nerve (orbit, temple & parietal areas), lasts for a few seconds and occurs at irregular intervals with no accompanying symptoms. Stabs may move from one area to another and can occur in those who suffer from migraines or cluster HA (on the same side). If the stab recurs persistently in the same area they must be investigated.
Cough HA = Headache precipitated by coughing or straining in the absence of any intracranial disorder.
Sudden onset lasting 1-30sec, brought on by coughing, straining or valsalva. Occurs more regularly in those over 40 and is associated with Arnold Chiari malformation. Can also be caused by vertebrobasilar or carotid diseases and aortic aneurysm – diagnostic neuroimaging plays a role in indentifying this.
Exertional HA = Precipitated by any form of exercise.
Pulsating HA lasting 5min-48hrs, brought on by or occurring after exertion. On first occurrence of this headache type it is mandatory to exclude subarachnoid haemorrhage and arterial dissection.
Sexual Intercourse HA = Precipitated by sexual activity, usually starting as a dull bilateral ache as sexual excitement increases and suddenly becoming intense at orgasm, in the absence of any intracranial disorder.
Hypnic HA = Attacks of dull headache that always awaken the patient from asleep. Develops only with sleep and wakes patient up. Lasts longer >15min after waking and occurs >15 times per month, occurs after 50years. No ANS symptoms and no more than 1 nausea/photophobia/phonophobia.
Usually bilateral, mild/moderate pain, lasting from 15-180mins.
Thunderclap = High-intensity headache of abrupt onset mimicking that of ruptured cerebral aneurysm. Sudden onset, reaching max intensity in <1min, lasting from 1hr-10days, does not occur regularly and is not associated with any other disorder. CSF must be checked and brain imaging carried out to rule out cause. Thunderclap headache is frequently associated with serious vascular intracranial disorders, particularly subarachnoid haemorrhage
Primary thunderclap headache should be the diagnosis only when all organic causes have been excluded.
http://ihs-classification.org/en/02_klassifikation/
With or without aura (without most common).
Without = Idiopathic recurring headache disorder with attacks lasting 4-72hours.
Unilateral, pulsating quality, moderate/severe intensity, aggravated by physical activity and associated with nausea/vomiting, photo- and phonophobia. Must have occurred on 5 occasions.
Caused by sensitivity of vessels in the brain to various triggers leading to vapid changes in vessel diameter – constriction followed by dilation = pulsating quality. Changes in blood composition and platelet function endogenously or environmentally play a role in triggering them. May be associated with the menstrual cycle.
With = Idiopathic, recurring disorder with attacks of neurological symptoms localised to the cerebral cortex or brain stem, usually developing over 5-20min and lasting 60min. HA, nausea, and/or photophobia follow the aura. HA may last 4-72hr or may be absent.
Typical aura = Unilateral visual disturbance, hemisensory symptoms, hemiparesis or dysphasia or any combination of these.
Regional cerebral blood flow is decreased (to area corresponding with symptoms), usually starting posteriorly and spreading anteriorly. Reduction in blow flow in usually above or at ischemic threshold and rarely below. Gradual transition to hyperaemia occurs in the same area (not related to the HA).
Can be difficult to distinguish from tension HA but are usually unilateral.
2. Tension-type headache (TTHA)
Recurrent episodes of HA lasting minutes to days. Typically pressing/tightening in quality, mild/moderate intensity, bilateral, not worsened with routine physical activity. Nausea and vomiting are absent but photo- and/or phonophobia may be present. Can be episodic or chronic, which can be extremely disabling. Peripheral pain mechanisms play a role in episodic TTHA, whereas central mechanisms are involved with chronic TTHAs.
Infrequent episodic TTHA = < 12/year. No nausea/vomiting. Some photo/phonophobia. 30min to 7days.
Frequent episodic TTHA = >12 but <180 days/year. No nausea/vomiting. Some photo/phonophobia. 30min to 7days. With or without pericranial muscle tenderness (temporalis, masseter, medial and lateral pterygoids, SCM, splenius capitis, sub-occipitals and trapezius).
Chronic TTHA = HA occurring >15days/month for more than 3months or >180days/year. (Episodic can progress to chronic). No nausea/vomiting. Some photo/phonophobia. 30min to 7days.
Exact mechanisms are unknown but they are related to involuntary tightening of muscles induced physically or mentally. Generally considered to be psychogenic but more severe types may also have a neurobiological basis.
Is the most common type of primary HA, occurring in 30-78% of the population
3. Cluster headache / chronic paroxysmal hemicrania
Cluster HA = Severe, unilateral pain that is orbital, supraorbital, temporal or any combination, lasting 15min to 3hrs, up to 8 times per day. Often associated with; unilateral conjunctival infection, lacrimation, nasal congestion, rhinorrhoea, forehead and facial sweating, miosis, ptosis, eyelid oedema and restlessness/agitation.
Occur in periods that may last weeks or months and are separated by periods of remission lasting months or years - 10-15% experience chronic symptoms without remission.
During a cluster period attacks may be provoked by alcohol, histamine or nitroglycerine. Pain can be excruciatingly intense with the patient unable to lie down. Pain invariably recurs on the same side.
Paroxysmal Hemicrania = Attacks with similar characteristics to cluster Has but more frequent, shorter lasting, more common in females and respond absolutely to indomethacin (NSAID).
At least 20 attacks of severe unilateral orbital/supraorbital/temporal pain lasting 2-30min. Associated with conjunctival infection, lacrimation, nasal congestion, rhinorrhoea, forehead and facial sweating, miosis, ptosis, eyelid oedema and restlessness/agitation. Five attacks per day.
4. Miscellaneous headaches not associated with structural lesion
Stabbing HA = Transient and localised stabs of pain in the head that occur spontaneously in the absence of organic disease of underlying structures or of the cranial nerves.
Predominantly felt in the distribution of the ophthalmic branch of the trigeminal nerve (orbit, temple & parietal areas), lasts for a few seconds and occurs at irregular intervals with no accompanying symptoms. Stabs may move from one area to another and can occur in those who suffer from migraines or cluster HA (on the same side). If the stab recurs persistently in the same area they must be investigated.
Cough HA = Headache precipitated by coughing or straining in the absence of any intracranial disorder.
Sudden onset lasting 1-30sec, brought on by coughing, straining or valsalva. Occurs more regularly in those over 40 and is associated with Arnold Chiari malformation. Can also be caused by vertebrobasilar or carotid diseases and aortic aneurysm – diagnostic neuroimaging plays a role in indentifying this.
Exertional HA = Precipitated by any form of exercise.
Pulsating HA lasting 5min-48hrs, brought on by or occurring after exertion. On first occurrence of this headache type it is mandatory to exclude subarachnoid haemorrhage and arterial dissection.
Sexual Intercourse HA = Precipitated by sexual activity, usually starting as a dull bilateral ache as sexual excitement increases and suddenly becoming intense at orgasm, in the absence of any intracranial disorder.
Hypnic HA = Attacks of dull headache that always awaken the patient from asleep. Develops only with sleep and wakes patient up. Lasts longer >15min after waking and occurs >15 times per month, occurs after 50years. No ANS symptoms and no more than 1 nausea/photophobia/phonophobia.
Usually bilateral, mild/moderate pain, lasting from 15-180mins.
Thunderclap = High-intensity headache of abrupt onset mimicking that of ruptured cerebral aneurysm. Sudden onset, reaching max intensity in <1min, lasting from 1hr-10days, does not occur regularly and is not associated with any other disorder. CSF must be checked and brain imaging carried out to rule out cause. Thunderclap headache is frequently associated with serious vascular intracranial disorders, particularly subarachnoid haemorrhage
Primary thunderclap headache should be the diagnosis only when all organic causes have been excluded.
http://ihs-classification.org/en/02_klassifikation/
Traumatic HAs
1. Associated with head trauma
Acute= Moderate/severe - HA with no typical characteristics. Head trauma with loss of consciousness >30min/GCS score <13/amnesia >48hr/ imaging showing brain lesion.
HA develops within 7days of trauma and resolves within 3months.
Mild - HA with no typical characteristics. No loss of consciousness or loss >30min/GCS >13/symptoms consistent with concussion.
Chronic = Often part of the post-traumatic syndrome which includes a variety of symptoms such as equilibrium disturbance, poor concentration, decreased work ability, irritability, depressive mood, sleep disturbances.
Persists for >3months.
2. Associated with neck trauma
Acute whiplash = HA with no typical characteristics, develops with 7 days of whiplash injury (associated with neck pain), last for <3months. Headache is very common in this post-whiplash syndrome as well as other extra-cervical symptoms. Evolution of these varies widely.
Chronic whiplash = As above. Lasts for >3months. Often part of post-traumatic syndrome. There is no good evidence that ongoing litigation, with settlement pending, is associated with prolongation of headache.
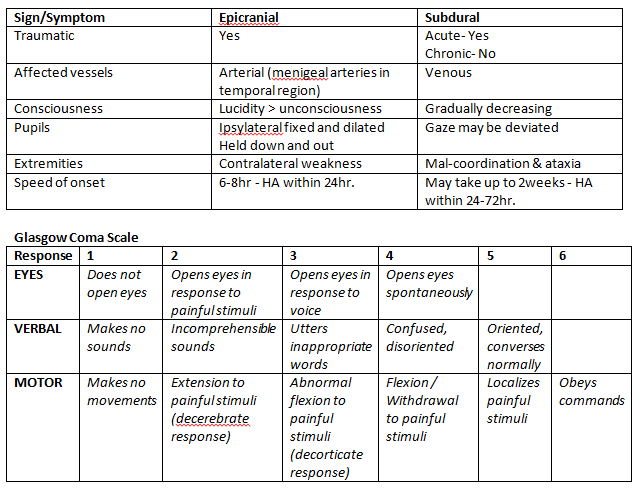
3. Associated with traumatic intracranial haematoma
Signs of raised ICP may be present (vomiting without nausea, ocular palsies, altered consciousness and papilloedema)
Epidural Haematoma (between skull and dura)= Acute onset HA, no typical characteristics. HA develops within minutes to 24hr post-trauma.
Bleeds are rapid as damage is usually arterial. Peak at 6-8hr post-trauma.
Patient may be lucid immediately following trauma, followed by unconsciousness. Compression of Ipsylateral fixed and dilated pupil held down and out (compression of CNIII and CN IV & VI are unopposed).
Contralateral weakness in extremities (pyramidal compression)
Contralateral loss of visual field (compression of post. Cerebral artery)
If medullary structures are compromised it can lead to cardiac arrest.
Confirmed by CT scan (bioconvex). Cannot expand past skull sutures.
Subdural Haematoma (between dura and arachnoid) = Acute onset HA, no typical characteristics. HA develops within 24-72hr.
With acute haematoma HA is overshadowed by issues of consciousness and focal signs. With chronic conditions HA may be the overriding symptom and should be considered esp. If the patient is elderly the HA is progressive and there is a degree of cognitive impairment.
Results from tears in bridging veins. Symptoms can appear immediately or take up to 2 weeks to develop. Gradually increasing HA and confusion.
Loss/fluctuating consciousness, irritability, seizure, pain, numbness, HA (fluctuating), dizziness, disorientation, amnesia, weakness/lethargy, nausea or vomiting, anorexia, slurred speech, ataxia, altered breathing, tinnitus, deviated gaze.
Confirmed by CT classically crescent shaped. An spread along inside of skull.
Acute= Moderate/severe - HA with no typical characteristics. Head trauma with loss of consciousness >30min/GCS score <13/amnesia >48hr/ imaging showing brain lesion.
HA develops within 7days of trauma and resolves within 3months.
Mild - HA with no typical characteristics. No loss of consciousness or loss >30min/GCS >13/symptoms consistent with concussion.
Chronic = Often part of the post-traumatic syndrome which includes a variety of symptoms such as equilibrium disturbance, poor concentration, decreased work ability, irritability, depressive mood, sleep disturbances.
Persists for >3months.
2. Associated with neck trauma
Acute whiplash = HA with no typical characteristics, develops with 7 days of whiplash injury (associated with neck pain), last for <3months. Headache is very common in this post-whiplash syndrome as well as other extra-cervical symptoms. Evolution of these varies widely.
Chronic whiplash = As above. Lasts for >3months. Often part of post-traumatic syndrome. There is no good evidence that ongoing litigation, with settlement pending, is associated with prolongation of headache.
3. Associated with traumatic intracranial haematoma
Signs of raised ICP may be present (vomiting without nausea, ocular palsies, altered consciousness and papilloedema)
Epidural Haematoma (between skull and dura)= Acute onset HA, no typical characteristics. HA develops within minutes to 24hr post-trauma.
Bleeds are rapid as damage is usually arterial. Peak at 6-8hr post-trauma.
Patient may be lucid immediately following trauma, followed by unconsciousness. Compression of Ipsylateral fixed and dilated pupil held down and out (compression of CNIII and CN IV & VI are unopposed).
Contralateral weakness in extremities (pyramidal compression)
Contralateral loss of visual field (compression of post. Cerebral artery)
If medullary structures are compromised it can lead to cardiac arrest.
Confirmed by CT scan (bioconvex). Cannot expand past skull sutures.
Subdural Haematoma (between dura and arachnoid) = Acute onset HA, no typical characteristics. HA develops within 24-72hr.
With acute haematoma HA is overshadowed by issues of consciousness and focal signs. With chronic conditions HA may be the overriding symptom and should be considered esp. If the patient is elderly the HA is progressive and there is a degree of cognitive impairment.
Results from tears in bridging veins. Symptoms can appear immediately or take up to 2 weeks to develop. Gradually increasing HA and confusion.
Loss/fluctuating consciousness, irritability, seizure, pain, numbness, HA (fluctuating), dizziness, disorientation, amnesia, weakness/lethargy, nausea or vomiting, anorexia, slurred speech, ataxia, altered breathing, tinnitus, deviated gaze.
Confirmed by CT classically crescent shaped. An spread along inside of skull.
Others!
Headache associated with cranial/cervical vascular disorder:
-TIA/Stroke – HA with focal neurological signs and changes in consciousness (TIA <24hr)
-Non-traumatic intracranial haemorrhage – Most commonly due to sub-arachnoid bleeds.
Intense, incapacitating HA of abrupt onset (thunderclap). Non-traumatic due to ruptured aneurysm. Unilateral, nausea, vomiting, consciousness disorder and nuchal rigidity. Less severe can be without associated symptoms. Neurosurgical emergency.
-Unruptured vascular malformation –
-GCA – Temporal HA, swollen tender scalp, increased CRP/ESR, jaw claudication, may have PMR.
Headache associated with non-vascular disorders:
- Increased CSF Pressure = Idiopathic, secondary to metabolic/toxic/hormonal causes, secondary to hydrocephalus.
Diffuse/constant pain, daily, worse with valsalva, papilloedema, enlarged blind-spot, CnVI palsy, visual filed defects.
- Decreased CSF Pressure = Post-LP HA, CSF Fistula, spontaneous.
Stiff neck, tinnitus, hypacusia, photophobia, nausea.
- Neoplasm = Directly – Progressive, localised, worse in morning, aggravated by changes in pressure. Indirectly – Associated with n/v, worse with physical activity/increase in ICP, attack-like episodes.
- Epileptic Seizure
- Arnold Chiari Malformation
Headache Associated with Substance/Substance withdrawal:
- Acute, overuse, adverse event (OD/allergic reaction), withdrawal.
Headache Associated with infection:
Intracranial Infection
- Bacterial Meningitis = Diffuse pain, increasing intensity, nausea/photophobia/phonophobia, stiff neck, generally unwell (fever, malaise). HA can be first sign.
- Non-Bacterial (lymphocytic) Meningitis = Acute onset, severe pain, nuchal rigidity, fever, nausea, photo- and/or phonophobia.
- Encephalitis = Diffuse pain, increasing intensity, nausea, photo- and/or phonophobia.
Systemic Infection
- Diffuse pain, increasing intensity, fever, general malaise, other signs of systemic infection, HA develops during infection and resolves within 72hr of TTT.
HIV/AIDS
- Dull and bilateral, variable onset, site and intensity, develops in close relationship to HIV/AIDS associated pathology.
Headache Associated with disorder of cranium, neck, eyes, ears, nose, sinuses, teeth, mouth, jaw or other facial/cranial structures:
- Cranium = Congenital abnormalities, fracture, tumour, metastasis.
- Neck = Cervicogenic HA. Clinical features such as neck pain, focal neck tenderness, history of neck trauma, mechanical exacerbation of pain, unilaterality, coexisting shoulder pain, reduced range of motion in the neck, nuchal onset.
- Eyes = Acute glaucoma, refractive errors (bad eyesight!), squint, ocular inflammation.
- Nose = Rhinosinusitis. Sinus HA.
- TMJ, Teeth.
3. Cranial Neuralgias
- Trigeminal = Unilateral pain limited to 1 or more division of CnV. Triggered by trivial things such as talking, shaving , eating, washing etc. Intense, sharp, superficial, stabbing pain with no neurological deficit. Come and go quickly.
- Glossopharyngeal = Transient stabbing pain in the ear, base of tongue, tonsilla fossa of beneath angle of jaw. Provoked by swallowing, talking and couching, may relapse and remit.
- Optic Neuritis = Dull pain behind one or both eyes, worse with eye movement, visual impairment (central or paracentral scotoma), pain precedes visual impairment by <4weeks.
- Herpes Zoster = Pain in distribution of nerve or nerve branch.
-TIA/Stroke – HA with focal neurological signs and changes in consciousness (TIA <24hr)
-Non-traumatic intracranial haemorrhage – Most commonly due to sub-arachnoid bleeds.
Intense, incapacitating HA of abrupt onset (thunderclap). Non-traumatic due to ruptured aneurysm. Unilateral, nausea, vomiting, consciousness disorder and nuchal rigidity. Less severe can be without associated symptoms. Neurosurgical emergency.
-Unruptured vascular malformation –
-GCA – Temporal HA, swollen tender scalp, increased CRP/ESR, jaw claudication, may have PMR.
Headache associated with non-vascular disorders:
- Increased CSF Pressure = Idiopathic, secondary to metabolic/toxic/hormonal causes, secondary to hydrocephalus.
Diffuse/constant pain, daily, worse with valsalva, papilloedema, enlarged blind-spot, CnVI palsy, visual filed defects.
- Decreased CSF Pressure = Post-LP HA, CSF Fistula, spontaneous.
Stiff neck, tinnitus, hypacusia, photophobia, nausea.
- Neoplasm = Directly – Progressive, localised, worse in morning, aggravated by changes in pressure. Indirectly – Associated with n/v, worse with physical activity/increase in ICP, attack-like episodes.
- Epileptic Seizure
- Arnold Chiari Malformation
Headache Associated with Substance/Substance withdrawal:
- Acute, overuse, adverse event (OD/allergic reaction), withdrawal.
Headache Associated with infection:
Intracranial Infection
- Bacterial Meningitis = Diffuse pain, increasing intensity, nausea/photophobia/phonophobia, stiff neck, generally unwell (fever, malaise). HA can be first sign.
- Non-Bacterial (lymphocytic) Meningitis = Acute onset, severe pain, nuchal rigidity, fever, nausea, photo- and/or phonophobia.
- Encephalitis = Diffuse pain, increasing intensity, nausea, photo- and/or phonophobia.
Systemic Infection
- Diffuse pain, increasing intensity, fever, general malaise, other signs of systemic infection, HA develops during infection and resolves within 72hr of TTT.
HIV/AIDS
- Dull and bilateral, variable onset, site and intensity, develops in close relationship to HIV/AIDS associated pathology.
Headache Associated with disorder of cranium, neck, eyes, ears, nose, sinuses, teeth, mouth, jaw or other facial/cranial structures:
- Cranium = Congenital abnormalities, fracture, tumour, metastasis.
- Neck = Cervicogenic HA. Clinical features such as neck pain, focal neck tenderness, history of neck trauma, mechanical exacerbation of pain, unilaterality, coexisting shoulder pain, reduced range of motion in the neck, nuchal onset.
- Eyes = Acute glaucoma, refractive errors (bad eyesight!), squint, ocular inflammation.
- Nose = Rhinosinusitis. Sinus HA.
- TMJ, Teeth.
3. Cranial Neuralgias
- Trigeminal = Unilateral pain limited to 1 or more division of CnV. Triggered by trivial things such as talking, shaving , eating, washing etc. Intense, sharp, superficial, stabbing pain with no neurological deficit. Come and go quickly.
- Glossopharyngeal = Transient stabbing pain in the ear, base of tongue, tonsilla fossa of beneath angle of jaw. Provoked by swallowing, talking and couching, may relapse and remit.
- Optic Neuritis = Dull pain behind one or both eyes, worse with eye movement, visual impairment (central or paracentral scotoma), pain precedes visual impairment by <4weeks.
- Herpes Zoster = Pain in distribution of nerve or nerve branch.
