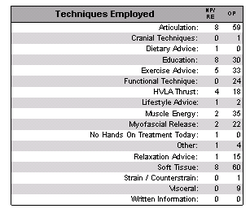
Techniques up to Spring term (including Christmas Break)
So, what was the impact of doing a visceral elective on my treatments, along with an additional course on the pelvis?
In the term where (and week of "holiday" after) I learnt the techniques, I performed 9 separate instances of visceral technique.
In the term where (and week of "holiday" after) I learnt the techniques, I performed 9 separate instances of visceral technique.
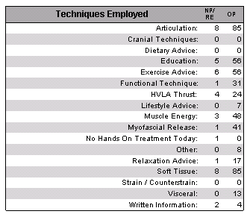
Techniques for the Spring term
Then, over the Spring term, there were thirteen separate instances.
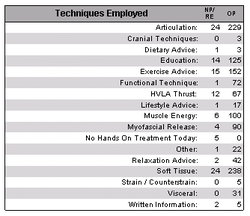
Techniques for all time!
And now, for all time, there are 31, so not even half-way through the final term I have performed 31-9-13=9 more lots of visceral technique already!
So it is definitely happening more. But to what end? For the most part, I use techniques relating to the diaphragm, to aid breathing mechanics, especially when considering rib function.
However, I am currently treating one patient for nocturia explicitly, and have definitely noticed an impact to palpation. However, how she responds to the treatment remains to be seen next week. At our last appointment, she was cautiously optimistic, but I am strongly aware that she may be so only to please me, and doing my best to find objective evidence to confirm or deny any changes.
In particular, if there are no subjective or objective changes at our next appointment, I am somewhat at a loss of how to intervene in the matter further as my perceived changes seem to have reached a conclusion where there is little more to do.
Nevertheless, the treatment was cautiously proposed to the patient as an experiment, after reading through her extensive file, where it was possible to find a timeline of pelvic damage and resetting with consequential beginnings of changes in bowel and bladder function. These initially seemed to subside, but then the bladder symptoms returned and set in over a few years, until they became her main ongoing complaint as an afterthought to all of her ongoing MSk problems which tend to respond nicely to treatment.
Fingers crossed!
So it is definitely happening more. But to what end? For the most part, I use techniques relating to the diaphragm, to aid breathing mechanics, especially when considering rib function.
However, I am currently treating one patient for nocturia explicitly, and have definitely noticed an impact to palpation. However, how she responds to the treatment remains to be seen next week. At our last appointment, she was cautiously optimistic, but I am strongly aware that she may be so only to please me, and doing my best to find objective evidence to confirm or deny any changes.
In particular, if there are no subjective or objective changes at our next appointment, I am somewhat at a loss of how to intervene in the matter further as my perceived changes seem to have reached a conclusion where there is little more to do.
Nevertheless, the treatment was cautiously proposed to the patient as an experiment, after reading through her extensive file, where it was possible to find a timeline of pelvic damage and resetting with consequential beginnings of changes in bowel and bladder function. These initially seemed to subside, but then the bladder symptoms returned and set in over a few years, until they became her main ongoing complaint as an afterthought to all of her ongoing MSk problems which tend to respond nicely to treatment.
Fingers crossed!
 RSS Feed
RSS Feed